Federal tax returns for 2018 are due April 15 in most states. With your filing, you can see how your taxes changed after the Tax Cuts and Jobs Act of December 2017.
You can compare your total taxes paid in 2018 to the amount paid in 2017. But your income may have changed, so instead you can compare your ratio of taxes to income in the two years. Middle-income filers received an estimated average tax cut of $780, and the ratio of their individual income, payroll, and excise taxes to income fell 9 percent (see top of table 1).
Polls show that the GOP tax cuts are not particularly popular. But that might be because of continued disinformation in the press. For example, in criticizing Steve Moore recently, Vanity Fair writer William D. Cohen said:
[Moore] started by saying that the tax law would reduce taxes for 90 percent of Americans. I objected strenuously. ‘Moore shouldn’t be allowed to do this anymore,” I said. “He’s been trying to do this for 35 years, talking about trickle-down economics for 25 years. He shouldn’t be allowed to do this anymore.’
I went on: ‘This isn’t a tax cut for 90 percent of the Americans. This is a tax increase for anybody who makes money paying ordinary income taxes. Maybe if you pay capital gains taxes, maybe like Donald Trump if you have a lot of partnership income, this could be a tax cut. But from both people who get a paycheck who have a W‑2, this would be a tax increase.’
What the heck? There were only minor changes to capital gains taxes in the law, and Cohen’s claim that most or all ordinary folks got tax increases is far off base. Moore’s claim that 90 percent received cuts is more accurate.
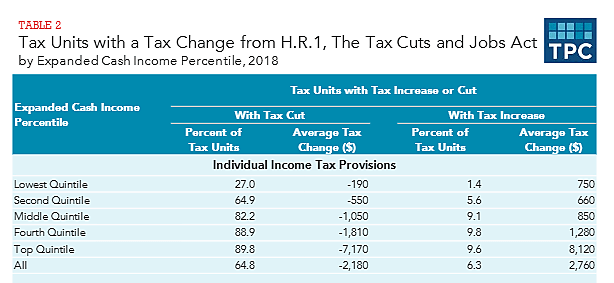
The table below from the Tax Policy Center (TPC) shows the share of households that received individual cuts in 2018 within five income groups (see top of table 2).
Overall, 65 percent of households received a tax cut and just 6 percent had an increase. However, the bottom two income groups, on net, do not pay any individual income taxes. The tax “cuts” for those two groups are mainly increases in refundable tax credits.
Looking at households that pay federal income taxes—those in the top three groups—more than 82 percent received an individual tax cut under the GOP tax law. If you include the effects of the corporate tax cuts, more than 90 percent of households in these tax-paying groups received a cut (see bottom of table 2).
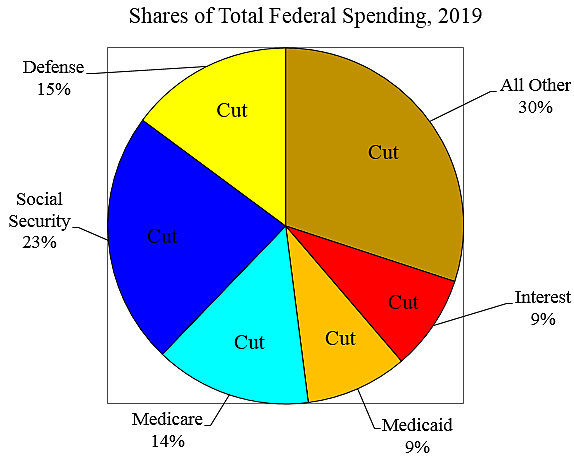
Numerous aspects of the GOP tax law were misguided, including the increased progressivity it created, as noted here and here. Furthermore, Republican efforts to increase spending on defense, farm subsidies, and many other things are grossly inconsistent with their tax-cutting agenda.
However, the vast majority of tax-paying households did in fact receive a tax cut under the GOP law, and Steve Moore should “be allowed” to say it.