ObamaCare requires each state to open its Medicaid program to all legal residents earning up to 138 percent of the federal poverty level. Supporters estimate this mandate will cost state governments little: the Kaiser Family Foundation’s worst-case-scenario estimates suggest that state Medicaid spending would rise by just 1.2 percent in New York and 5.1 percent in Texas between 2014 and 2019.
In a new working paper titled, “Estimating ObamaCare’s Effect on State Medicaid Expenditure Growth,” Cato Institute Senior Fellow Jagadeesh Gokhale shows that those estimates are generally far too low. Gokhale finds that all of the five most-populous states — California, Florida, Illinois, New York, and Texas, which account for roughly 40 percent of U.S. population — will struggle to cope with rising Medicaid spending even without ObamaCare’s Medicaid mandate. But ObamaCare significantly increases that burden on four of them:
In its first year of full implementation (2014), ObamaCare will increase spending on Medicaid by 9.0 percent in Florida, 22.2 percent in Illinois, 6.4 percent in New York, and 13.5 percent in Texas. Spending in California is projected to be smaller by about 3 percent.
The cost grows over time. The following chart shows the burden that ObamaCare’s Medicaid mandate will impose on these states over the first 10 years of full implementation:
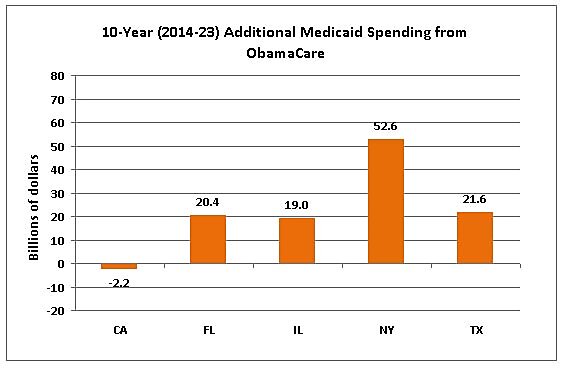
Compared to a world without ObamaCare, state Medicaid spending will decline by 3 percent in California, but increase by 17.1 percent in Florida, 28.1 percent in Illinois, 16.5 percent in New York, and 12.9 percent in Texas over the first 10 years of full implementation.
On a per-taxpayer basis, ObamaCare’s Medicaid mandate is also highly inequitable:
for every $1 in costs imposed on each working-age Texas adult, Floridians and New Yorkers will pay about $1.50, Illinoisans will pay $3.60, while Californians will save a small amount (about 3 pennies).
Gokhale explains that the Kaiser Family Foundation’s projections are lower because they assume that ObamaCare’s individual mandate will not significantly increase enrollment among people who were eligible for Medicaid but not enrolled under the pre-ObamaCare rules. Consistent with other research, Gokhale assumes the individual mandate will encourage people to enroll in Medicaid even if they would not face financial penalties for being uninsured.
Update (3/3/11): The chart and text were updated to reflect corrected numbers.
