The government’s approach toward treating people with substance use disorder is degrading and dehumanizing. It stigmatizes people who are suffering from a compulsive behavioral disorder. We don’t treat people with other physical or mental health disorders this way.
In fact, roughly 3 million people in the U.S. suffer from opioid use disorder. More than 500,000 are dependent on heroin. Yet only 400,000 Americans are accessing methadone treatment.
But with overdose deaths exceeding 100,000 per year and roughly 90 percent involving illicit fentanyl, some lawmakers in Congress are finally starting to think outside the box. Last year, Senators Edward D. Markey (D‑MA) and Rand Paul (R‑KY) and Representatives Donald Norcross (D‑NJ) and Don Bacon (R‑NE) introduced legislation that would have allowed some physicians to prescribe take‐home methadone to patients with substance use disorder, as physicians have been doing for more than 50 years in the U.K., Canada, and Australia. The bill failed to pass in the 117th Congress.
On March 6, 2023, the same authors reintroduced the Modernizing Opioid Treatment Access Act in the new Congress, which is essentially identical to last year’s bill.
While doctors can and do prescribe methadone for pain, the Drug Enforcement Administration (DEA) and the Substance Abuse and Mental Health Services Administration (SAMHSA) impose stringent regulations on methadone treatment for addiction. Patients must travel daily—sometimes long distances—to Opioid Treatment Programs (OTPs), queue up outside the OTPs, and take the methadone in the presence of clinic staff.
DEA’s and SAMHSA’s onerous regulations make it difficult for organizations to start and maintain OTPs. These organizations must also battle local NIMBYism, as people don’t want centers that “attract drug addicts” in their communities. As a result, a quarter of the U.S. population lacks an OTP in their county. There are no OTPs at all in the state of Wyoming.
During the COVID public health emergency, SAMHSA relaxed several regulations so people with substance use disorder could access these medications while minimizing the risk of contracting the virus. For example, SAMHSA allowed OTPs to give a 28‐ day supply of take‐home methadone to “stable” patients and a 14‐day supply to “less stable” patients.
Further, the agency permitted OTPs to operate vans that can go out to the patients where they live. To deal with pandemic‐ related OTP staffing problems, SAMHSA allowed people to receive “interim treatment” from OTPs (daily methadone but without the counseling and other services typically offered by OTPs) for up to 180 days. SAMHSA allowed certain OTP follow‐up visits to use telemedicine.
In July 2022, a study published in JAMA Psychiatry by researchers led by the National Institute on Drug Abuse, National Institutes of Health, and the Centers for Disease Control and Prevention reported that the emergency take‐ home methadone program “was not associated with harms” and “add[ed] evidence to support take‐ home treatment for opioid use disorder.”
After numerous reports that the relaxed regulations did not result in misuse or diversion of methadone into the black market, SAMHSA decided to extend the relaxed rules until one year after the President officially declared the public health emergency over.
On December 16, 2022, SAMHSA published a Notice of Proposed Rulemaking (NPRM) and solicited comments. The NPRM would make all the emergency measures permanent.
I submitted my comment to the agency. In it, I argued the relaxed rules were a step in the right direction, but that I and many others have long argued that health care practitioners—especially primary care providers interested in treating substance use disorder—should be allowed to prescribe take‐home methadone to treat their patients with substance use disorder as they have been doing for decades in other countries.
Furthermore, pilot programs in the U.S. have shown that this approach can be safe and effective in American communities. A 2018 article in the New England Journal of Medicine pointed to the success of this and other pilot programs. It called on Congress to pass legislation allowing health care practitioners to prescribe methadone as MAT to their patients with substance use disorder. In January 2020, the National Academy of Science, Engineering, and Medicine (NASEM) made a similar plea. I have made this argument as well. In my comment to SAMHSA, I stated:
The only way to completely destigmatize people with substance use disorder, and thus facilitate their access to care and improve the likelihood of recovery, is to remove the regulations and restrictions unique to opioid treatment programs. This includes rules affecting the use of telemedicine technology. Licensed health care practitioners should be able to prescribe opioid agonists such as methadone, as well as the partial agonist buprenorphine, to people with substance use disorder the same way the government allows them to specify beta blockers to treat hypertension and insulin to treat diabetes. In short, if the Substance Abuse and Mental Health Services Administration seriously wants to destigmatize people with substance use disorder, it can start by destigmatizing how they receive treatment.
The Modernizing Opioid Treatment Access Act begins the de‐stigmatization process by increasing access to methadone treatment for people with substance use disorder by allowing patients to receive treatment in doctors’ offices and clinics in the community. However, as Zoe Adams, MD et al. commented in Health Affairs when the legislation was introduced last year, the bill has shortcomings. A significant drawback is that the legislation only permits methadone prescriptions from “addiction medicine physicians or addiction psychiatrists who hold a subspecialty board certification in addiction medicine from the American Board of Preventive Medicine, a board certification in addiction medicine from the American Board of Addiction Medicine, a subspecialty board certification in addiction psychiatry from the American Board of Psychiatry and Neurology, or a subspecialty board certification in addiction medicine from the American Osteopathic Association.”
If lawmakers want to increase access to methadone treatment profoundly, they should allow primary care practitioners, including licensed Family Nurse Practitioners (FNPs), to treat patients with methadone. Treating substance use disorder is complicated. It requires practitioners to commit seriously to developing close relationships with their patients, taking the time for deep discussions, and monitoring them closely. Not every primary care practitioner will feel competent or interested in treating patients with substance use disorder. They will refer such patients to appropriate practitioners. But allowing all interested primary care providers to engage in methadone‐assisted treatment will significantly expand the options and access to patients needing care.
Unfortunately, not nearly enough doctors in the US meet those requirements to increase access to the degree the bill’s sponsors envision. The following table lists the number of physicians registered in each specialist category by state as of March 6, 2023.
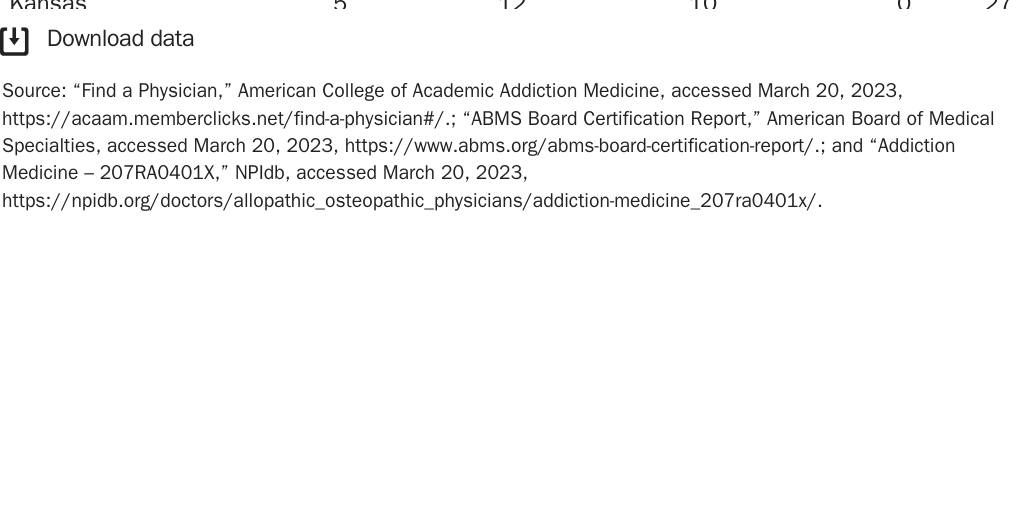
Even if all the physicians can accept new patients, there are not enough of them to serve the millions of Americans with opioid use disorder who are not currently getting treated. Some states have very few qualifying physicians. For example, Wyoming has only five.
Another drawback is that the bill limits the amount that doctors may prescribe to their patients to a supply of “not more than 30 days.” One would hope that after the fiasco of 38 states cementing in statute opioid prescribing guidelines based on the scientifically questionable and now‐revised 2016 opioid guidelines — which inflicted catastrophic harm on chronic pain patients — lawmakers would avoid legislating how doctors practice medicine.
Lawmakers should not tie clinicians’ hands. Doctors treating substance use disorder best know how, when, and how much to prescribe, especially to their long‐term patients. As Adams and her colleagues stated, “Take-home methadone dosing should be decided by science, clinicians, and patients.”
Despite these shortcomings, Senators Markey and Paul, Representatives Norcross and Bacon, and their co-sponsors deserve praise for taking this important and worthy first step outside the box. Hopefully, it will be the first of many new measures in the right direction.
(Cato intern Anchal Kumar contributed to this blog post.)
