There are few forecasts more important for public finance and public policy than the projected growth in health expenditures. Health spending may grow because of price inflation or improvements in the quality of medical care, but the future rate of growth is unknown. Health spending is equal to roughly 18 percent of gross domestic product (GDP), and federal spending on health care exceeded $1 trillion in 2018. The sheer size of this sector means that forecasted growth rates have a significant impact on public planning. In addition to its impact on public budgeting, forecasts affect private-sector planning and legal disputes, such as damages in personal injury cases.
The Office of the Actuary (OACT) for the Centers for Medicare and Medicaid Services (CMS) produces one such forecast for medical care spending growth. The most recent forecast projected an average annual growth rate of 5.5 percent for the period 2018–2027. For several reasons, however, the true growth rate can exceed this forecast. For example, one important limitation of the OACT forecast is that it is restricted to current law and does not assume any potential legislative changes. To the extent that there are potential policy changes on the horizon that might raise the cost of health care, this institutional limitation will create a downward forecast bias.
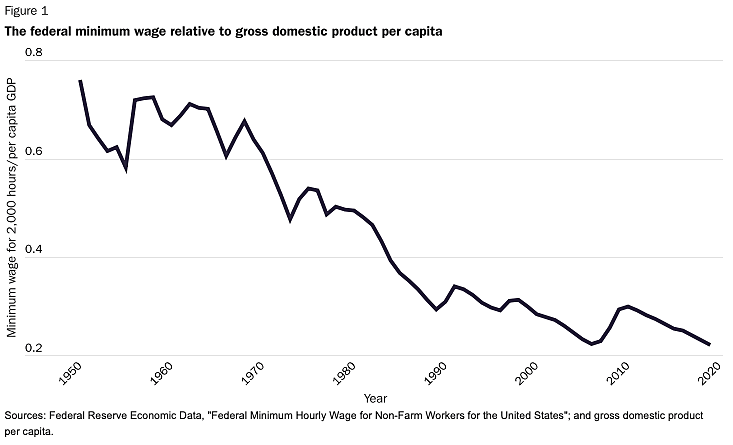
I illustrate this problem by demonstrating the relationship between one such potential policy change and an important segment of medical expenses. Specifically, I show an extremely strong relationship between changes in state-level minimum wage and price increases in costly components of medical care, such as home health aides, homemaker services, adult daycare, assisted living facility residency, and nursing home care. I do this using data collected from tens of thousands of providers and using a variety of statistical tests. The relationship is highly robust. While many people in these industries make more than the minimum wage, the minimum wage is still a significant component of the aggregate production costs for long-term care. I find that, among states, a $1 increase in the minimum wage predicts an increase in annual costs for homemaker services and home health aide services of roughly 7.5 percent, adult daycare services and assisted living services of 10.2 percent, and nursing home care of 17–18 percent. The sensitivity of long-term care costs to the minimum wage is crucial in part because the federal minimum wage has shrunk considerably relative to GDP in recent years. My results suggest that this erosion, demonstrated in Figure 1, has been a limiting factor in the growth rate of costs for these components.
Perhaps as a result, there has been a recent push to raise the federal minimum wage. The Democratic Party platform calls for raising the federal minimum wage by more than 100 percent from the current level of $7.25 to $15. The majority of candidates running for the presidential nomination of the Democratic Party support this policy. The overwhelming majority of Americans—both Republican and Democrat— support increasing the minimum wage, and a clear majority desires an increase to $15.
The OACT projections for nursing care facilities and continuing care retirement communities (5 percent spending growth in aggregate, 4.1 percent per capita) and other health, residential, and personal care expenditures (5.7 percent in aggregate, 4.8 percent per capita) ignore this major potential shock. While a $15 minimum wage is not guaranteed, the most scientifically accurate forecast should incorporate the likelihood. My results suggest that a $15 minimum wage would have a dramatic impact on the cost of long-term care. Moreover, a rising minimum wage is just one of the potential policy changes on the horizon that raise the anticipated growth rate of health care costs.
NOTE:
This research brief is based on Daniel Shoag, “Health Care Spending Projections and Policy Changes: Recognizing the Limitations of Existing Forecasts,” Harvard Kennedy School Faculty Research Working Paper Series no. RWP19-022, June 2019, https://www.hks.harvard.edu/publications/health-care-spending-projectionsand-policy-changes-recognizing-limits-existing.

About the Author
Harvard Kennedy School and Case Western Reserve University

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.