Dr. Rahul Gupta, the White House director of the Office of National Drug Control Policy, stated the Biden administration would be “prioritizing harm-reduction practices because these are proven, cost-effective and evidence-based methods that work to save lives.”1 Overdose prevention centers (OPCs) are a successful harm-reduction strategy that has been saving lives in 16 developed countries—including the United States, where such facilities operate in defiance of the law.
OPCs, also known as safe consumption sites or drug consumption rooms, began in Europe in the mid-1980s.2 Governments and harm-reduction organizations now operate OPCs in much of Europe, Canada, Mexico, and Australia. Unfortunately, a federal law that prosecutors and harm-reduction opponents call the “crack house” statute (21 U.S.C. Section 856) makes them illegal in the United States.3
Some OPCs in the United States operate in the shadows. Underground OPCs have been providing services since at least 2014. More recently, state and local officials have been approving OPCs in defiance of federal law.
This policy brief reviews how OPCs are an effective, mainstream harm-reduction strategy. Congress should stop standing in the way of local harm-reduction organizations that seek to reduce overdose deaths by establishing OPCs.
The Worsening Overdose Crisis
Since President Richard Nixon declared a “war on drugs” in 1971, U.S. drug policy has focused relentlessly on interdicting and reducing the illicit drug supply and, in recent years, pressuring doctors to reduce the number of controlled substances they prescribe. Nevertheless, since the late 1970s, drug overdose deaths in the United States have continued to mount, exceeding 107,000 in 2021, according to the Centers for Disease Control and Prevention.4 Drug prohibition makes using illicit drugs more dangerous because drug users cannot be sure of the purity and dosage of drugs they obtain on the black market, which puts them at a greater risk of accidentally overdosing. What drug policy scholars call “the iron law of prohibition” magnifies the problem: as law enforcement grows more vigorous, so too does the potency of prohibited substances.5 Concealing and smuggling drugs that are more potent is easier. Drug cartels are producing and smuggling increasingly potent analogs of fentanyl, and users often mix them with stimulants to create deadly “cocktails.” This trend has led modelers to predict a massive wave of new overdose deaths.6
Featured Video
Against that backdrop, some U.S. policymakers have recently begun to embrace harm-reduction strategies after long resisting that approach. Harm-reduction strategies begin with the realistic and nonjudgmental premise that society never has been and will never be drug-free. Akin to the credo of the medical profession—“First, do no harm”—harm reduction seeks to avoid measures that exacerbate the harms the black market already inflicts on nonmedical users and to focus strictly on the goal of reducing the spread of disease and death from drug use.7
Syringe services programs (SSPs, also known as needle exchange programs) are a common harm-reduction strategy that federal public health agencies promote.8 Such programs primarily provide clean needles and syringes to people who inject drugs (PWID). Clean syringes effectively reduce the spread of infectious diseases but do not reduce overdoses. In fact, one study found that SSPs effectively reduced new cases of HIV but correlated with an increase in overdose deaths.9 In recent years, many SSPs have therefore sought to reduce overdoses by also distributing fentanyl test strips and the opioid overdose antidote naloxone.10 Although those products can reduce and reverse opioid overdoses, they are likely less effective if PWID are using them in unsupervised settings. For example, users who are injecting when they are alone may have difficulty using naloxone to reverse an overdose.
How OPCs Work
OPCs have more ambitious goals. They furnish PWID with sterile syringes and needles. They allow PWID to inject illicitly obtained drugs in a clean, indoor clinical setting, out of public view, where users are free from harassment and the risks of theft and physical or sexual assault. Onsite health care professionals have naloxone available to treat overdoses and can refer patients for medical treatment and rehabilitation. The centers provide equipment for drug users to test their drugs for fentanyl and other contaminants. Drug users must return syringes after using them to prevent passing or selling used needles and syringes to others. In recent years, many drug users in the United States have switched from injecting to inhaling (snorting or smoking) drugs, as in much of the rest of the world.11 With inhalation, drug users can better adjust the amount of drug they consume to reach the desired effect and avoid taking too large a dose, as often happens when injecting. OPCs often provide clean and safe inhalation devices to those clients. Most facilities require users to spend time in “chill-out rooms” to allow the drug’s initial effects to subside so the user is less impaired when leaving the site. OPCs often provide showers and other facilities and connect users to social services.12 Many clients respond to the nonjudgmental, caring atmosphere of safe consumption sites by seeking treatment and other social services.13
The Growth of OPCs
During alcohol prohibition, speakeasies provided a secret and safer place to consume an illegal drug. OPCs got their start as the speakeasies of today’s war on drugs. The world’s first professionally staffed—yet illegal—consumption room opened in Rotterdam, the Netherlands, in the early 1970s. In 1986, the illegal consumption site Contact Netz began operating in a café in Bern, Switzerland. The Swiss government eventually removed legal obstacles to Contact Netz serving clients older than age 18, making it the first legal overdose prevention center in the world. The Dutch government officially approved such centers in 1996.14
During the 1990s and early 2000s, more legal centers opened in Australia, Canada, Germany, Luxembourg, the Netherlands, Norway, Spain, and Switzerland.15 Germany’s first drug consumption room (DCR) opened in Berlin in 1994. Australia opened its first facility in 2001, the Uniting Medically Supervised Injection Centre (MSIC) in the Kings Cross district of Sydney (or MSIC–Sydney). Canada opened its first overdose prevention center, Insite, in the Downtown Eastside district of Vancouver in 2003.
At least one illegal OPC has been operating somewhere in the United States since 2014. Researchers have reported in the peer-reviewed medical literature—without revealing the site’s name or location—that the site is reducing overdoses.16 In Seattle, underground OPCs sometimes operate out of apartments.17 In Philadelphia, the city council voted to permit a private OPC, Safehouse, in 2019, but the U.S. Department of Justice threatened to arrest the principals and staff, and the OPC never opened.18 In July 2021, Rhode Island governor John McKee signed legislation that legalized privately funded OPCs.19 And on November 30, 2021, the mayor of New York City announced that two private nonprofit OPCs had opened—one in East Harlem and one in Washington Heights—and both continue to provide services.20 The U.S. Department of Justice has not yet intervened in Rhode Island or New York City. On August 22, 2022, California governor Gavin Newsom vetoed a bill that would have created OPC pilot programs in San Francisco, Oakland, and Los Angeles.21
The OPC Harm-Reduction Record
Strong evidence indicates that OPCs reduce the transmission of HIV and hepatitis, prevent overdose deaths, reduce public injections, reduce the volume of shared or discarded syringes, and increase the number of drug users entering treatment programs.22 A 1996 report on injecting rooms in Switzerland concluded the following: “Injecting rooms have enabled the adoption of less hazardous injecting practices, reduced the number of overdose deaths, minimised [sic] the nuisance to the community of injecting in public places, and probably reduced HIV transmission. The Centres are well‐tolerated in Swiss communities. Some [intravenous drug users] have entered treatment as a result of attending injecting rooms.”23
A 2011 retrospective analysis of the 25 OPCs then operating in Germany found OPCs significantly reduce “problems related to the open drug scene in cities,” “significantly contribute to limiting the spread of infectious diseases such as hepatitis and HIV,” and “make a decisive contribution for survival assistance and risk minimization when consuming illegalized drugs.”24
Critics in the United States view such sites as endorsing intravenous drug use and other illegal activities.25 Those concerns are understandable, but the evidence shows OPCs save lives by reducing overdose deaths and have likely saved lives by reducing the spread of deadly diseases and violence against drug users.
The Global Experience with OPCs
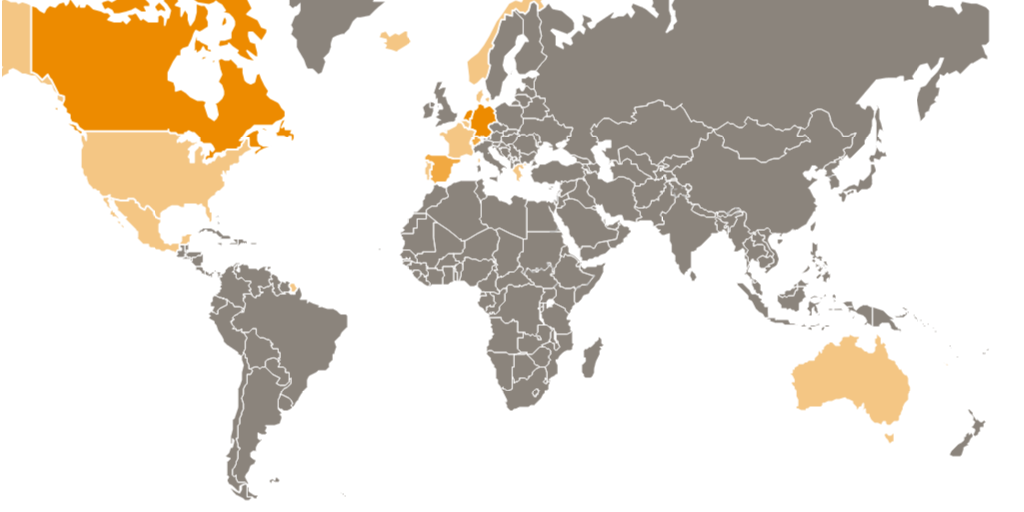
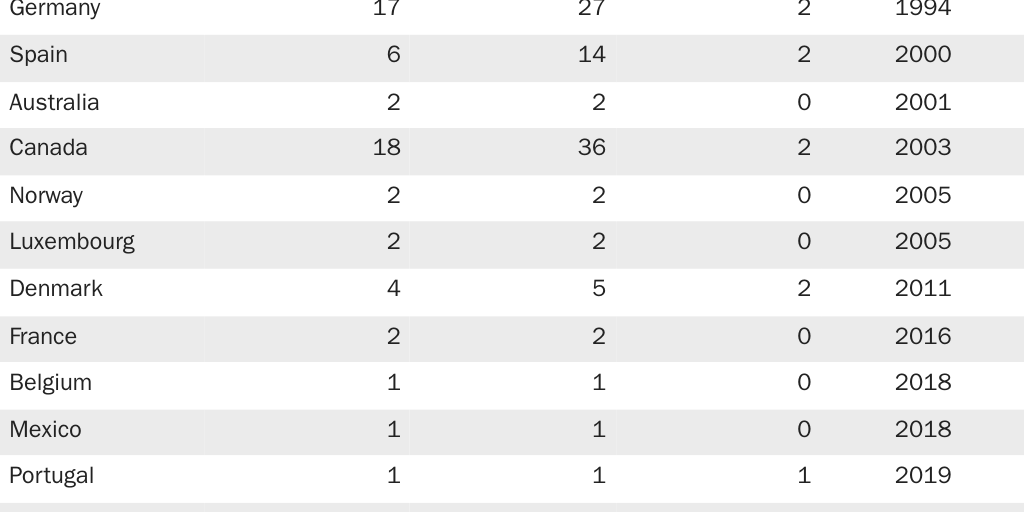
Worldwide, 147 OPCs provide services in 91 communities in 16 countries as of August 2022 (Figure 1). Table 1 lists the countries where fixed and mobile OPCs operate, along with the year each established its first facility. Table 1 includes two countries—the United States and Belgium—where OPCs are illegal under national law.
Writing in the New England Journal of Medicine, researchers report that the underground OPC that has been operating in the United States since 2014 oversaw 10,514 injections and reversed 33 overdoses from 2014 through 2019.26 New York City has been defying federal law ever since the New York City Department of Health opened two OPCs on November 30, 2021.27 New York City OPC staff reported they had reversed 230 overdoses as of April 3, 2022.28
The Belgian Drug Law of February 24, 1921, prohibits “providing a premise” to consume a controlled substance.29 Nevertheless, Belgium’s first OPC opened in Liege in 2018 and continues to serve people who inject drugs. City and regional authorities subsidize this OPC in defiance of federal law.30
Also in 2018, the private company Integracion Social Verter, A.C. (Verter) opened La Sala, an unsanctioned OPC in Mexicali, Mexico, close to the U.S.-Mexico border. This is the first OPC in Latin America and one of only four OPCs in the world exclusive to women.31 Though the government does not officially sanction the facility, the program’s coordinator claims the site is legal.32
Featured Event
Switzerland
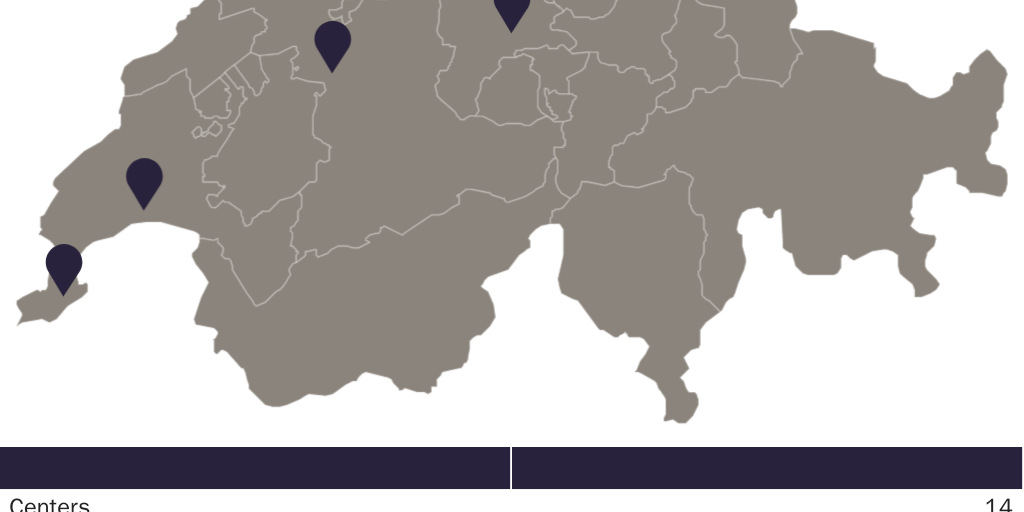
The first unofficial consumption room opened in Zurich in 1981, primarily to prevent PWID from falling victim to the HIV/AIDS pandemic.33 The strategy was unpopular with authorities in many Swiss cities. Despite initial skepticism, the Zurich site resulted in safer and more hygienic injections, decreased the number of syringes bought on the street, and decreased sexual assault. In 1986, the government allowed Contact Netz, an OPC in Bern, to operate under new regulations that allowed safe injection facilities for heroin users older than age 18. The OPC in Bern trains nurses, social workers, and medical professionals to administer and manage such sites.34 Figure 2 shows the current distribution of OPCs in Switzerland, along with the injection and overdose data for Contact Netz.
Switzerland’s drug policy rests on four pillars: harm reduction, treatment, prevention, and control/law enforcement. A 1997 national referendum on the four pillars policy garnered 70 percent support. In 2008, the revised Narcotic Act codified the four pillars policy.35
The Netherlands
The first unsanctioned OPC opened in Amsterdam in the 1970s, but after several complaints, Amsterdam closed all OPCs in 1986.36 Dutch policymakers began reopening OPCs in the 1990s. As of April 2022, 26 OPCs are now operating in 21 communities in the country. OPCs in the Netherlands do not systematically record the number of users who visit and consume drugs, which limits data availability; however, facility staff estimate OPCs serve 5 to 30 clients daily.37
Germany
Germany’s first DCR opened in Frankfurt in 1992, primarily to reduce public displays of intravenous drug use. The country now has 27 fixed and 2 mobile OPCs in 17 communities. Policymakers justify those sites based on their role in preventing overdoses and disease. From 1992 to 2012, OPCs in Germany documented 191,729 injections, averaging 550 per day, with zero fatalities onsite.38
Australia
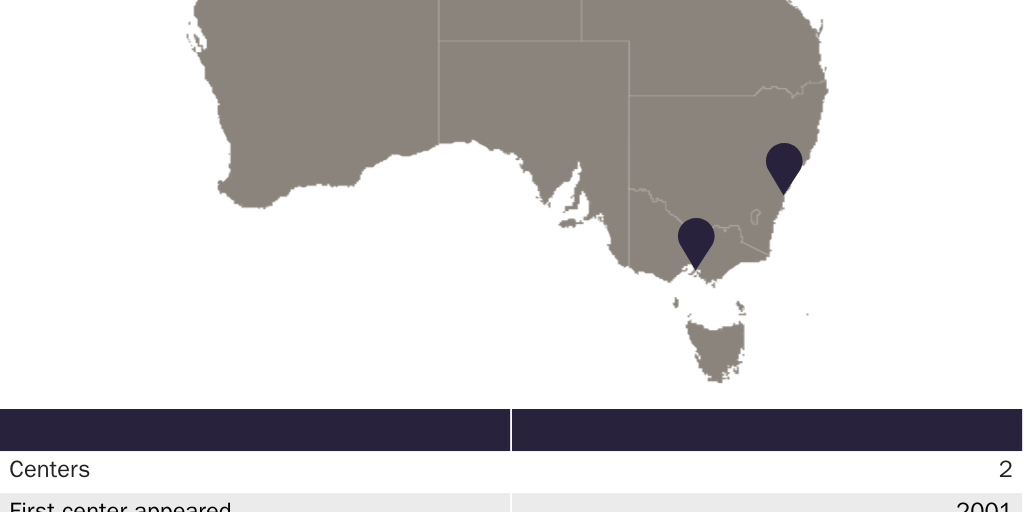
Drug laws in the states of New South Wales and Victoria permit OPCs to operate in Sydney and Melbourne. The country has two OPCs, called Medically Supervised Injection Centres (MSICs). Australia’s first site, Uniting, opened in Sydney in 2001.39 Between May 2001 and April 2022, staff supervised 1.237 million injections at the site.40 Half of the OPC’s clients reported they regularly injected drugs in public.41 Uniting targeted “hidden populations” of PWID who are unlikely to seek treatment elsewhere.42 The second site, North Richmond Community Health MSIC, in Melbourne, opened in June 2018.43 In its first 18 months, the site supervised 116,802 injections and managed 3,200 overdoses with zero deaths.
Figure 3 shows OPC locations in Australia and provides data for Uniting MISC–Sydney.
Luxembourg
Luxembourg’s first OPC, Abrigado, opened in Luxembourg City in 2005. Abrigado reported more than 73,000 supervised injections in 2017. A second OPC, for which no data are yet available, opened in 2019. Neither of the Luxembourg OPCs have had any fatalities.
Portugal and Spain
Portugal decriminalized all drugs in 2001, which also legalized drug consumption facilities. Yet it wasn’t until 2019 that the city council of Lisbon initiated Portugal’s first OPC, a mobile unit.44 Portugal now has one fixed and one mobile OPC, both in Lisbon.
In Spain, private consumption of illicit drugs is not a crime, but public consumption is a “serious breach” of the Law on the Protection of Citizens;45 therefore, consuming drugs in OPCs is not illegal. Spain has had OPCs since 2000 and currently has 14 fixed and 2 mobile OPCs.
France
Supervised injection rooms began as a medical experiment in Marseilles in 2011.46 The results led the French government to permit OPCs in 2016. In 2021, France’s health minister announced the goal of creating a network of OPCs throughout the country. The country currently has two fixed OPCs—one in Paris and one in Strasbourg.47
Norway
Norway opened its first OPC in 2005 after the legislature enacted the “Syringe Room Law,” which legalized heroin injection at sites with adequate supervision. On January 1, 2019, the legislature passed the “User Room Law,” expanding the types of narcotics (previously only heroin) and the consumption methods (previously only injecting) permitted in OPCs. Norway currently has two OPCs: one in Oslo and one in Bergen. At the end of August 2020, Oslo’s site expanded to include a dedicated inhalation room to respond to the growing number of drug users who snort, smoke, or otherwise inhale their drugs. Staff at that site are working to change users’ method of drug intake from injection to inhalation to support safer drug consumption. Figure 4 shows the locations of OPCs in Norway, with data from Oslo.

Denmark
OPCs began in Denmark in 2011, but the Danish government didn’t fully remove legal prohibitions on OPCs until the Danish parliament legalized DCRs in June 2012.48 The country currently has five fixed and two mobile OPCs in four locations and has never experienced fatalities.
Canada
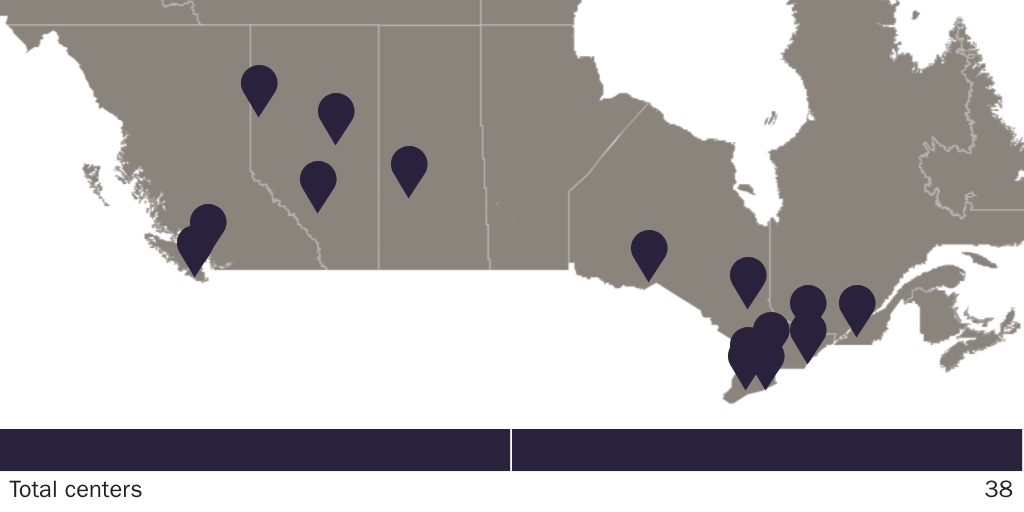
Canada has the highest number of OPCs worldwide, with 38 (36 fixed and 2 mobile) sites in 18 cities. None of Canada’s facilities have ever reported fatalities. In 2003, in Vancouver, Insite became Canada’s first legal site and is the source of most existing research on Canada’s OPCs. Aside from preventing lethal overdoses, Canada’s OPCs help prevent the spread of hepatitis C and HIV. They also provide other health care services for PWID. A study by the Vancouver Area Network of Drug Users found that “removing structural and environmental barriers that constrain access” to OPCs was pivotal “in establishing safer injecting routines.”49 Figure 5 shows the locations of OPCs in Canada and the most recently available data from Insite.
Iceland and Greece
Iceland’s supreme national parliament legalized OPCs in May 2020.50 Its first center, a mobile unit, began operating in 2022.
Greece’s parliament approved OPCs in 2019.51 The sites must obtain a license from the Ministry of Health and must keep a registry of clients. A fixed facility opened in Greece in 2022.
Policy Recommendations
OPCs are currently saving lives throughout the developed world. The U.S. Congress should remove federal barriers to creating them.
Ideally, Congress should end drug prohibition and devolve regulatory authority to the states, as it did when it repealed alcohol prohibition in 1933.52 Federally legalizing all drugs would allow harm-reduction organizations to operate facilities where people can consume drugs more safely. An added benefit is that legal, competitive markets combined with product liability tort laws would make drug use safer by holding drug makers and sellers accountable if they mislead their customers or if proper use of their products harms consumers. As with alcohol, some consumers would develop substance use disorder. As with alcohol addiction, however, policymakers and the public would be more likely to view substance use disorder as a private health matter, and the elimination of a stigma would make seeking and getting help easier for people with addiction.
A second-best solution would be for Congress to decriminalize all drugs, as Portugal did in 2001.53 Under decriminalization, the government would not punish users for possessing or using illicit substances or drug paraphernalia, including using them in OPCs. Because the manufacture and sale of drugs remains illegal, however, users would still obtain drugs through the black market and would not be sure of the drug dosage and purity. Drug decriminalization is, therefore, not as safe for users as legalization. Still, decriminalizing all drugs removes obstacles to OPCs and other harm-reduction strategies.
A third-best solution would be for Congress to repeal 21 U.S.C. Section 856, the so-called “crack house” statute. Repealing the statute would get the federal government out of the way of local harm-reduction organizations that are ready to establish and run OPCs.
Finally, if Congress cannot repeal the “crack house” statute, it should at an absolute minimum amend existing federal law so harm-reduction organizations can establish and run OPCs.
Conclusion
OPCs have a more-than-30-year track record of preventing overdose deaths, HIV and hepatitis, and other diseases, and of helping people with substance use disorder find treatment. As of August 2022, 147 OPCs are providing services in 91 communities in 16 countries. They continue to gain acceptance as an effective tool for reducing the dangers of using drugs obtained through the increasingly deadly black market. Congress should remove federal barriers to OPCs in the United States.

About the Author


This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.