In his March 1, 2022, State of the Union address, President Biden focused the nation’s attention on a “national mental health crisis.”1 Before the COVID-19 pandemic, mood disorders and suicidal thoughts and behaviors had been rising at alarming levels for years.2 The pandemic and government-mandated lockdowns increased isolation, anxiety, and despair while also reducing access to mental health services. According to a 2022 Harris Poll conducted for the National Council on Mental Wellbeing, approximately 40 percent of Americans said they could not get mental health services in the past 12 months, particularly services requiring drug-based therapy.3
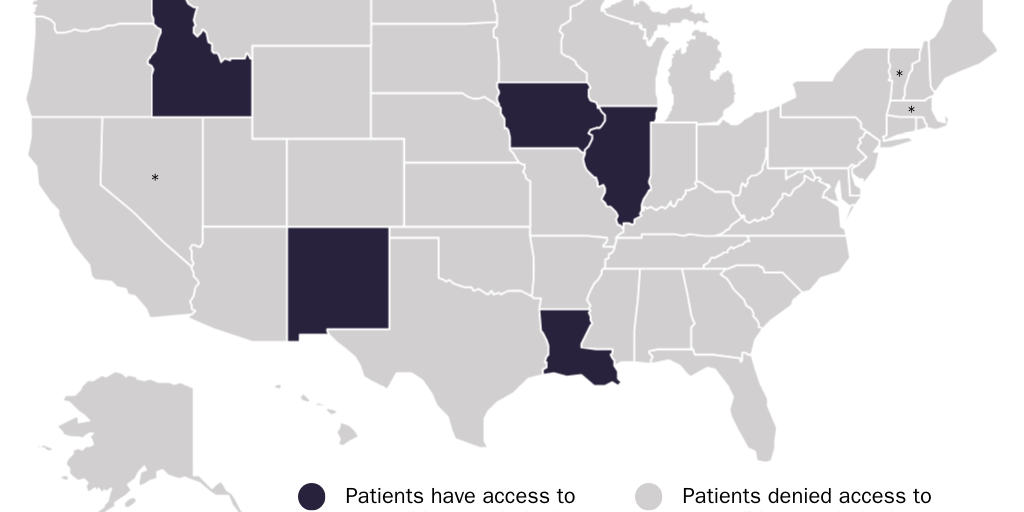
Clinical psychologists could be playing a greater role in meeting those needs. Some federal agencies, five states, and the territory of Guam authorize competent clinical psychologists to prescribe medications that treat mental illness by affecting mood and mental functions.
Unfortunately, most states prohibit competent clinical psychologists from prescribing such medications. To help address the mental health crisis, state lawmakers should expand the scope of practice of competent clinical psychologists to include prescribing.
The Problem
Mental illness is a serious and growing problem in the United States. The National Institute of Mental Health estimates that 52.9 million, or nearly 1 in 5, adults in the United States live with mental illness.4 In 2021, nearly 48,000 U.S. residents died from suicide.5 Suicide is the second-leading cause of death among people aged 10–34 in the United States.6 The U.S. Department of Veterans Affairs reports that veterans die from suicide at twice the rate of non-veterans. The rate is nearly three times higher for veterans aged 18–34.7 People with mental health disorders often develop substance use disorders, which contributes to the skyrocketing increase in drug overdose deaths.8 Reports of anxiety, depression, feeling isolated, self-harm, and suicidal thoughts among young adults and adolescents began to increase beginning around 2012.9 After rising 35 percent from 1999 to 2018, suicide rates declined 5 percent through 2020, though provisional data show suicide rates returning to pre-pandemic levels, increasing by 4 percent from 2020 to 2021.10
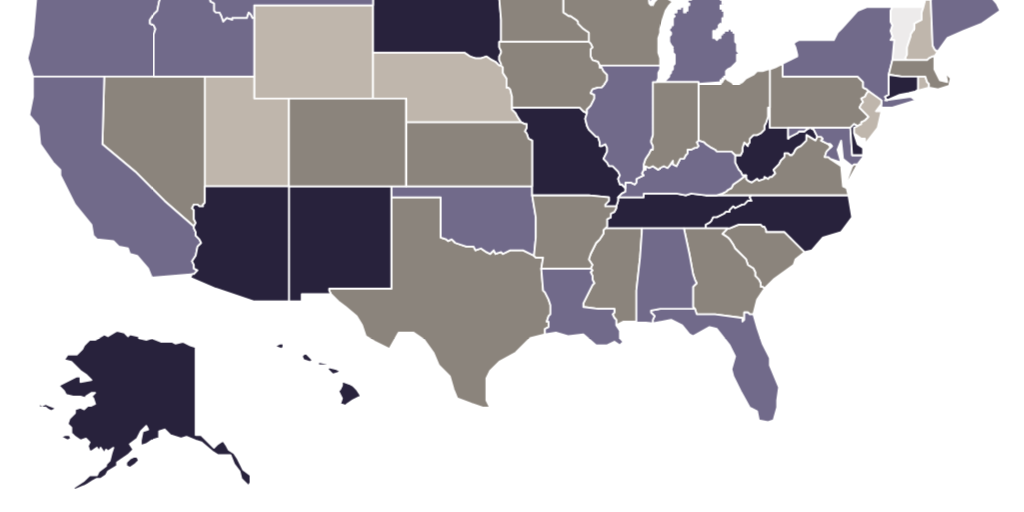
Research indicates that growing numbers of patients are seeking treatment for mental illness, yet supply is unable to meet existing needs. The Centers for Disease Control and Prevention estimates that 23.2 percent of adults aged 18–44 received mental health services during the past 12 months in 2021, an increase from 18.5 percent in 2019.11 A 2020 report by the Kaiser Family Foundation concluded that the United States has only enough psychiatrists to meet 26 percent of the population’s needs. The federal government estimates the need for mental health services and designates certain areas of each state to be “health provider shortage areas” if the number of psychiatrists cannot meet that level of need. Figure 1 presents, on a statewide basis, Kaiser Family Foundation estimates of how much of that need the existing stock of psychiatrists could meet. Lending credence to claims of mental health care shortages is the fact that states erect considerable barriers to entry that restrict the supply of mental health services.
The Role of Clinical Psychologists in Mental Health Care
Clinical psychologists diagnose and treat mental health disorders using various methods of talk therapy. States require clinical psychologists to obtain a doctoral degree in clinical psychology (PhD or PsyD) from a state-approved institution. Satisfying the requirements that states impose to become a clinical psychologist typically takes 8–12 years; many states also require a postdoctoral fellowship, which can add 1–2 years.12
In general, clinical psychologists do not prescribe medications. If they believe antidepressants, mood stabilizers, or other medications would facilitate therapy, they refer patients to a prescribing practitioner. Depending on the state, prescribing practitioners can include physician assistants and nurse practitioners in addition to physicians.13
Usually, the prescribing practitioner of choice is a psychiatrist. Psychiatrists are medical doctors with extensive training in using medication to treat mental illness. Nowadays, psychiatrists function primarily as prescribers. One survey found that only about 10.8 percent of psychiatrists offered any talk therapy.14
Psychiatrists are costly and in short supply. Initial consultations with a psychiatrist can cost as much as $500, and follow-up visits can range from $100 to $300 per hour.15 Roughly half of psychiatrists don’t accept insurance.16 Per capita, there are about twice as many clinical psychologists as psychiatrists in the United States (30 versus 16.6 per 100,000 people) and nearly three times as many in rural areas (9.1 versus 3.4 per 100,000 people).17 Many rural counties lack an adequate number of psychiatrists.18 Patients must often travel long distances to see psychiatrists to whom their clinical psychologists refer them.
Clinical psychologists can also refer patients to other prescribing practitioners, including non-specialist physicians and, where state law permits, physician assistants and nurse practitioners. States allow these clinicians to prescribe antidepressants, mood stabilizers, and antipsychotics even though they often lack expertise in these medications. Referring clinical psychologists often advise and support these practitioners on which medication(s) to prescribe.19 (See Appendix.) In some cases, clinical psychologists may have more expertise about these medications than the prescribing practitioners they advise.
One Potential Solution: Prescribing Psychologists
“Prescribing psychologists” (RxPs) became a distinct psychology specialty in the United States in 1991 when the Department of Defense (DOD) trained 10 clinical psychologists to prescribe medications in a six-year trial program at certain military bases.20 Military service can take a severe psychological toll on personnel. In 1989, in an effort to expand mental health care to military personnel, Congress directed the DOD to “establish a demonstration pilot training program under which military psychologists may be trained and authorized to issue appropriate psychotropic medications under certain circumstances.”21 The DOD developed a two-year program of classroom instruction and clinical training. The federal government asserts the authority to develop its own clinician categories and training programs for health professionals who work exclusively within federal agencies, including in cases where those clinicians’ activities may not comply with state law.22
An American College of Neuropsychopharmacology panel consisting of three psychiatrists and three clinical psychologists, each of whom “had research and clinical experience” and “served as directors of training programs,” continually evaluated the program. The panel found that RxPs “filled critical needs, and they performed with excellence wherever they were placed.” Seven of the RxPs worked with psychiatrists. An eighth collaborated somewhat with “a staff psychiatrist [who] was less experienced in psychopharmacology than the [RxP] graduate—and openly admitted this.” The remaining RxPs did not collaborate with psychiatrists. One worked with primary care physicians, and the other worked with other psychologists. Among the graduates, “eight out of 10 were serving as chiefs or assistant chiefs of an outpatient psychology clinic or a mental health clinic.” Most had broad latitude to prescribe, with “no significant formulary restrictions.” The panel considered the few restrictions the graduates faced to be “unfounded and unreasonable.” Half of the graduates “advanced to independent provider status”; the panel disagreed with the reflexive denial of independent practice to other graduates. Importantly, the panel noted, “there have been no adverse effects associated with the practices of these graduates” in part because “they have shown impressively that they knew their own weaknesses, and that they knew when, where, and how to consult” with more-knowledgeable clinicians. The panel concluded, “it seems clear … that a 2‑year program—one year didactic, one year clinical practicum that includes at least a 6‑month inpatient rotation—can transform licensed clinical psychologists into prescribing psychologists who can function effectively and safely in the military setting to expand the delivery of mental health treatment to a variety of patients and clients in a cost effective way.”23
The U.S. General Accounting Office likewise reviewed the program. It concluded that the RxP graduates
seem to be well integrated at their assigned military treatment facilities … generally serve in positions of authority, such as clinic or department chiefs … treat a variety of mental health patients; prescribe from comprehensive lists of drugs, or formularies; and carry patient caseloads comparable to those of psychiatrists and psychologists at the same hospitals and clinics. Also … the clinical supervisors, providers, and officials we spoke with at the graduates’ current and prior locations—as well as a panel of mental health clinicians who evaluated each of the graduates—were complimentary about the quality of patient care provided by the graduates.24
Importantly, the RxPs “reduc[ed] the time patients must wait for treatment and [increased] the number of personnel and dependents who can be treated for illnesses requiring psychotropic medications.”25
Since that demonstration project, other federal agencies have recognized, and allowed patients to benefit from access to, prescribing psychologists. The Indian Health Service and the Commissioned Corps of the U.S. Public Health Service have removed barriers to competent clinical psychologists prescribing medications to their patients.26 Today, some of those pioneer RxPs are still prescribing and training other RxPs in the DOD and these other federal agencies. As of 2017, the DOD, the U.S. Public Health Service, and the Indian Health Service employed approximately 30 prescribing psychologists.27
Some state and territorial governments have also recognized the potential of prescribing psychologists. In 1999, the territory of Guam eased barriers to competent clinical psychologists prescribing medications. New Mexico became the first state to do so in 2002. Since then, Idaho, Louisiana, Illinois, and Iowa have followed suit.28 According to Dr. Beth Rom-Rymer of the American Psychological Association, there were approximately 222 active prescribing psychologists across the United States as of mid-2022.29
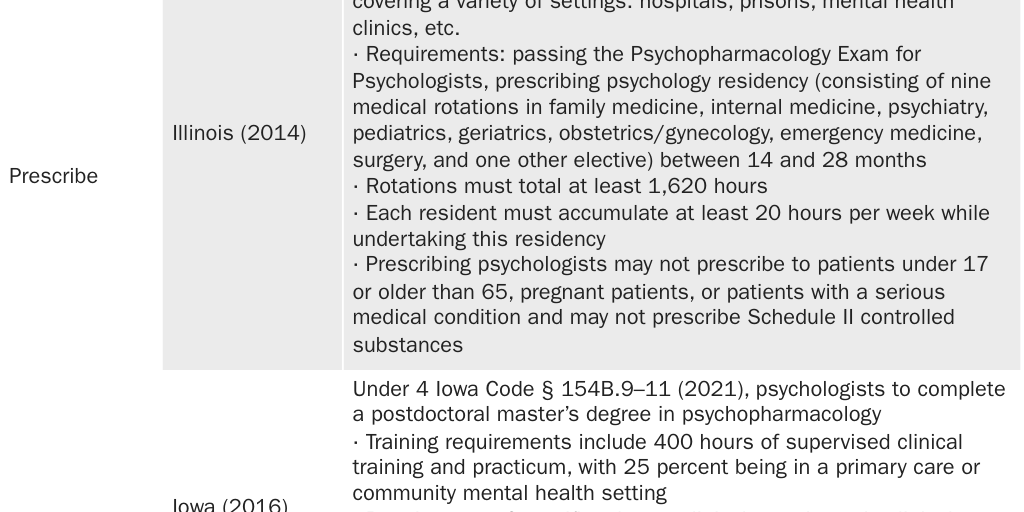
These states still impose substantial requirements on RxPs. Requirements include completing specialized instruction and training, acquiring a master’s degree in clinical psychopharmacology, and/or passing a national standardized exam, all on top of receiving a doctorate in clinical psychology. (See Figure 2 and Appendix.)
Even these requirements may be excessive. Illinois requires RxPs to pass the national standardized Psychopharmacology Exam for Psychologists (PEP) and to complete nine medical rotations (i.e., apprenticeships with medical doctors) accruing at least 1,620 hours of clinical experience within a span of 14–28 months. It is not immediately clear how rotations in, for example, obstetrics/gynecology and surgery enhance the quality of care of prescribing psychologists. The DOD recognized the potential for overtraining RxPs.30 As its program progressed, the DOD shortened and tailored medical school courses in anatomy, biochemistry, endocrinology, histology, microscopic pathology, and other subjects to meet the needs of prescribing psychologists.31
Indeed, these states require RxPs to receive more training and evaluation in knowledge, diagnosis, and treatment of mental health disorders (including medication treatment) than they require medical doctors to receive. States do not require primary care doctors to pass the PEP. Yet they do not restrict primary care doctors’ ability to prescribe psychotropic medications. Incongruously, in some cases, states require RxPs who did pass the PEP to coordinate care with a primary care physician who did not pass the PEP to obtain a conditional certification before they can prescribe independently.
The 45 states with complete bans on psychologists prescribing medications impose regulations that reduce access to mental health care and leave patients less safe. They reduce access by limiting the number of competent mental health practitioners who can prescribe medications. They leave patients less safe by allowing clinicians with less training to prescribe psychotropic medications but prohibiting clinical psychologists with more training from meeting that need. States permit primary care doctors, general surgeons, orthopedic surgeons, and other surgical specialists to prescribe psychotropic medications despite the fact that they have little knowledge or experience treating mental health problems. Those 45 states incongruously allow clinicians with less expertise to prescribe while prohibiting those with more expertise from prescribing. They prohibit RxPs who have passed a national exam on pharmacology from prescribing but impose no barrier to prescribing by medical doctors, and in some cases by nurse practitioners and physician assistants, who have not passed that exam.
Because the number of RxPs remains small, little data exist regarding how they prescribe relative to other health care professionals. The evidence to date suggests RxPs prescribe similarly to or more conservatively than psychiatrists. The American College of Neuropsychopharmacology panel found that in the DOD program, “The diagnoses made and the medications prescribed by the graduates … essentially mirrored what psychiatrists did with the same population, and, in fact, they differed little from the private practices of the psychiatrists on the Evaluation Panel.”32 One study in 2020 found that prescribing psychologists differ from psychiatrists and other health care practitioners in that they more often integrate prescribing medications with talk therapy. The study found that RxPs reduced the dosage or removed at least one medication for 57.8 percent of new patients who were already on medication. Nonprescribing mental health practitioners sometimes refer their patients to RxPs to prescribe medication. RxPs saw 35.8 percent of their patients for this reason. Nevertheless, the analysis found that only 0.8 percent of RxP patients’ sessions lasted 15 minutes or less, compared to psychiatrists, with whom 21.5 percent of visits were 15 minutes or less.33
Recommendations
State lawmakers should remove regulatory barriers that block competent clinical psychologists from prescribing medications to their patients.
Ideally, states should repeal licensing laws and accredit third-party certifying bodies to perform licensing boards’ functions. Such organizations review applicants’ education and experience to certify that they are competent to provide various types of mental health services.34 Existing third-party certifying organizations equipped to evaluate RxPs include the American Board of Clinical Pharmacology, the American Board of Psychiatry and Neurology, the American Board of Professional Psychology, and the American Society of Clinical Psychopharmacology.35 Even the American Psychiatric Association (which represents psychiatrists) and the American Medical Association (which represents medical doctors) could develop their own standards and certifications for RxPs to compete with those of other third-party organizations. RxPs could apply to one or more certifying organizations.
States should also enact laws recognizing practitioner licenses from other states and territories. Such laws should not require that practitioners reside in the state. This would enable licensed RxPs from the five states and Guam to provide talk therapy and prescribe medications to patients in the other states. In 2019, Arizona became the first state to recognize out-of-state occupational and professional licenses. Unfortunately, licensees must permanently reside in Arizona.36
As a second-best solution, states should work within existing law to reduce barriers to competent psychologists prescribing medications. Lawmakers should go even further than Idaho, Illinois, Iowa, Louisiana, and New Mexico have. States that require a master’s degree in clinical psychopharmacology (MSCP) should remove requirements that prescribing psychologists obtain that degree only after obtaining a doctorate in clinical psychology; competent RxPs might also obtain an MSCP either before or at the same time as they obtain a doctorate. States should remove barriers to RxPs who have trained through apprenticeships and educational programs other than MSCP programs, if they pass the national PEP exam and provide convincing evidence of knowledge and experience. As the DOD did, states should eliminate requirements that RxPs undergo unnecessary didactic instruction and should tailor such requirements to what prescribing psychologists will face in their practices. States should likewise eliminate clinical-experience requirements, such as obstetrics/gynecology and surgery rotations, that are not relevant to prescribing psychologists’ practices.
Lawmakers should not assume that existing educational paths or other paths that they might imagine are the only ways to produce competent prescribing psychologists. States should make licensing criteria flexible enough to accommodate educational innovations that academics, practitioners, and policymakers cannot foresee. For example, while an MSCP is one educational path RxPs can take, it is not the only path.
As a third-best solution, states should emulate New Mexico’s approach to regulating prescribing psychologists. New Mexico has the fewest barriers of the five states in which competent clinical psychologists currently prescribe. The state requires RxPs to acquire at least 450 hours of postdoctoral didactic instruction and 400 hours of clinical experience in clinical psychopharmacology. New Mexico avoids extraneous didactic and clinical experience requirements. The state prefers American Psychological Association–accredited postdoctoral programs but approves graduates of nonaccredited programs on a case-by-case basis. Graduates must also pass the national standardized PEP to receive a two-year provisional license. The state allows RxPs to practice independently but only after a primary care provider supervises them for two years. New Mexico’s regulations may still be unnecessarily burdensome, but applying them nationwide would dramatically expand access to vital mental health services.
Lobbyists for the incumbent prescribing professionals both reliably oppose efforts to remove these barriers and reliably support onerous or inflexible requirements for RxPs.37 Lawmakers should avoid enacting needlessly burdensome licensing requirements that protect incumbent prescribers from competition at the expense of patients.
Conclusion
Medication can be vital to the treatment of many mental illnesses. Because most states license only physicians (and, in some states, nurse practitioners and physician assistants) to prescribe these medications, it can be difficult for many people with mental illnesses to access affordable therapy that coordinates talk therapy with medication therapy.
Government-imposed barriers to entry restrict access to mental health professionals who are competent to prescribe medications. Prescribing clinical psychologists have a nearly 30-year track record of providing skilled, comprehensive mental health care to people with mental illnesses. Amid growing mental health needs and a shortage of mental health resources, state lawmakers should prioritize removing barriers to psychologists prescribing medications. Doing so can increase the supply of competent mental health prescribers and reduce the costs and inconvenience of mental health care.

About the Author


This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.